|
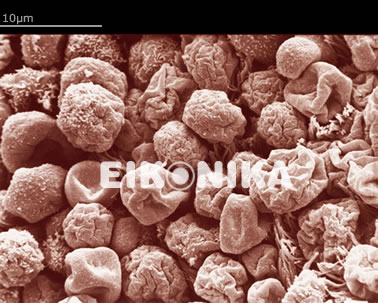
 endometrium before pinopode appearance (cycle day 18) endometrium before pinopode appearance (cycle day 18) |
|
|
In assisted reproduction (IVF), implantation failure after embryo transfer is a frequent and disappointing event.
A major and often neglected cause for this failure may be disturbances of the receptivity of the endometrium (the internal lining of the womb or uterus).
We have developed a clinical method to assess the endometrial receptivity as follows:
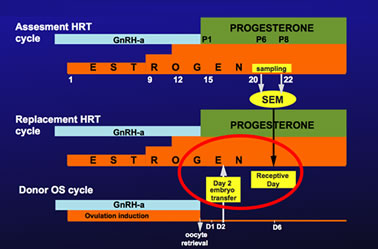
The patients go through a trial cycle where two samples are taken from the womb on cycle days 20 and 22.
The samples are examined under the scanning electron microscope to detect the 'pinopodes', characteristic markers of uterine receptivity. |
| |
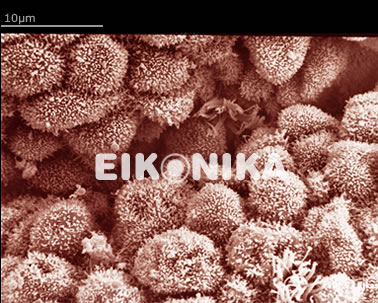
If pinopodes (developing, fully developed or regressing) are detected, we note the cycle day they form.
This information helps to better synchronize the time of embryo transfer with the womb.
A day six blastocyst should match with an endometrium containing fully developed pinopodes.
If pinopodes are detected in the first biopsy we advice embryo transfer earlier in the cycle.
If pinopodes are detected in the second biopsy we advice embryo transfer later in the cycle.
|
|
|
|
| |
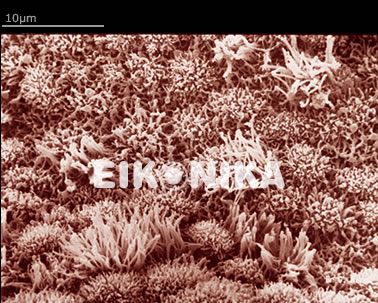
tweb.jpg) infected endometrium with red and white blood cells infected endometrium with red and white blood cells |
|
|
In many cases very few or no pinopodes are detected and the endometrium may display a variety of abnormalities that have to be treated accordingly.
The most frequently occurring abnormality is chronic infection, called endometritis.
It can be totally asymptomatic but may cause repeated implantation failure or pregnancy loss.
Endometritis may elude many diagnostic procedures, yet it is easily detected by SEM.
Endometritis is often difficult to cure, may require prolonged medication and in many cases a repeat biopsy after treatment is required to confirm that infection has been eliminated.
|
| |
 hyperestrogenized endometrium with micropolyp
hyperestrogenized endometrium with micropolyp |
|
|
Another common abnormality is a hyperplastic endometrium. In mild cases we advise modification of hormone administration while more severe cases may need curettage and progestin treatment.
Other abnormalities include atrophy or hormone imbalance that can be treated hormonally.
Endometrial defects are very common, particularly in patients with unexplained infertility.
These defects cannot be cured by IVF and if they are the only cause of infertility, IVF is not needed.
Our method of evaluating the endometrium has helped many patients with repeated implantation failures to achieve pregnancy, with or without IVF.
[publication 5, 7-10, 12-15, 17-26, 28, 30-33 and 36] |